
Transversus Abdominis Plane (TAP) Block Guide
TAP blocks target the intercostal nerves in the abdominal wall (thoracolumbar nerves T6–L1) to provide somatic analgesia (skin, muscle, parietal peritoneum) of the anterolateral abdomen
Coverage and Dermatomes
The TAP block anesthetizes the anterolateral abdominal wall on one side by blocking the ventral rami of T6–L1 (thoracolumbar spinal nerves) that run between the internal oblique (IO) and transversus abdominis (TA) muscle layers. It produces a band of unilateral abdominal wall analgesia roughly between the costal margin (upper abdomen) and the inguinal ligament (lower abdomen) on the side of the block
Because the block is confined to the fascial plane, it provides somatic pain relief (incisional and abdominal wall pain) but does not directly block visceral pain from internal organs. The parietal peritoneum (lining of abdominal cavity) is also anesthetized, which helps alleviate peritoneal irritation pain. In summary, a successful TAP block covers approximately T6/7 through L1 dermatomes of the anterior and lateral abdominal wall (including the skin, muscles, and parietal peritoneum of that region).
Indications and Surgical Uses
TAP blocks are typically part of a multimodal analgesia regimen to reduce opioid requirements and improve patient comfort after abdominal surgery. They can be performed preemptively (before incision) or at the end of surgery under ultrasound guidance. In patients with contraindications to neuraxial blocks (e.g. coagulopathy), TAP blocks (including continuous catheters) offer an alternate means of abdominal analgesia.
TAP blocks are indicated for postoperative analgesia after a variety of abdominal surgeries, especially those involving incisions in the lower thoracic or upper lumbar dermatomes. Common examples include:
- Appendectomy (RLQ incision) and cholecystectomy (RUQ incision)
Unilateral TAP block provides analgesia for these lateral abdominal incisions.
- Cesarean section, hysterectomy (e.g. total abdominal hysterectomy), and open prostatectomy
Bilateral TAP blocks can cover midline lower abdominal incisions (e.g. Pfannenstiel).
- Umbilical or ventral hernia repairs
Often require bilateral TAP blocks for midline incisions.
- Laparoscopic abdominal surgeries (e.g. laparoscopic appendectomy, cholecystectomy, bariatric surgery)
TAP block helps with trocar site and referred shoulder pain by numbing abdominal wall.
- Nephrectomy or renal transplant (flank incisions)
A posterior or lateral TAP block can be used for analgesia in lieu of epidural.
- Exploratory laparotomy
Bilateral TAP blocks for midline laparotomy incision analgesia.
- Abdominoplasty and iliac crest bone graft harvest
TAP blocks can provide analgesia for the abdominal wall/flank incisions.
Technique (Ultrasound-Guided TAP Block)
Patient Positioning: The TAP block is often performed with the patient in the supine position. For a lateral approach, some providers prefer a slight lateral decubitus position (side to be blocked up) to widen the space, but supine is feasible in most cases.
Probe Selection and Placement: Use a high-frequency linear ultrasound probe (hockey-stick or linear array) for adequate resolution of the abdominal wall layers. Place the probe in a transverse orientation on the anterolateral abdominal wall between the costal margin and iliac crest, along the midaxillary to anterior axillary line (for the lateral TAP approach). Ensure the probe is oriented such that you visualize the abdominal wall in cross-section (transverse axial view).
Ultrasound Landmarks: Identify the three muscle layers of the abdominal wall on the ultrasound image:
• From superficial to deep: the external oblique (EO) muscle (most superficial lateral abdominal muscle), the internal oblique (IO) muscle beneath it, and the transversus abdominis (TA) muscle as the deepest layer. These muscle layers appear as distinct hypoechoic (dark) bands separated by bright hyperechoic fascial lines on ultrasound.
• Deep to the TA muscle/fascia, you will see a layer of pre-peritoneal fat and then the peritoneum and bowel (often moving with peristalsis) deeper in the image. It is important to identify the peritoneal line to avoid puncturing it.
• The target plane for injection is the fascial plane between the IO and TA muscles, known as the transversus abdominis plane (TAP). In this plane run the segmental nerves (intercostal nerves T6–T11, subcostal T12, and iliohypogastric/ilioinguinal L1) which we aim to anesthetize.
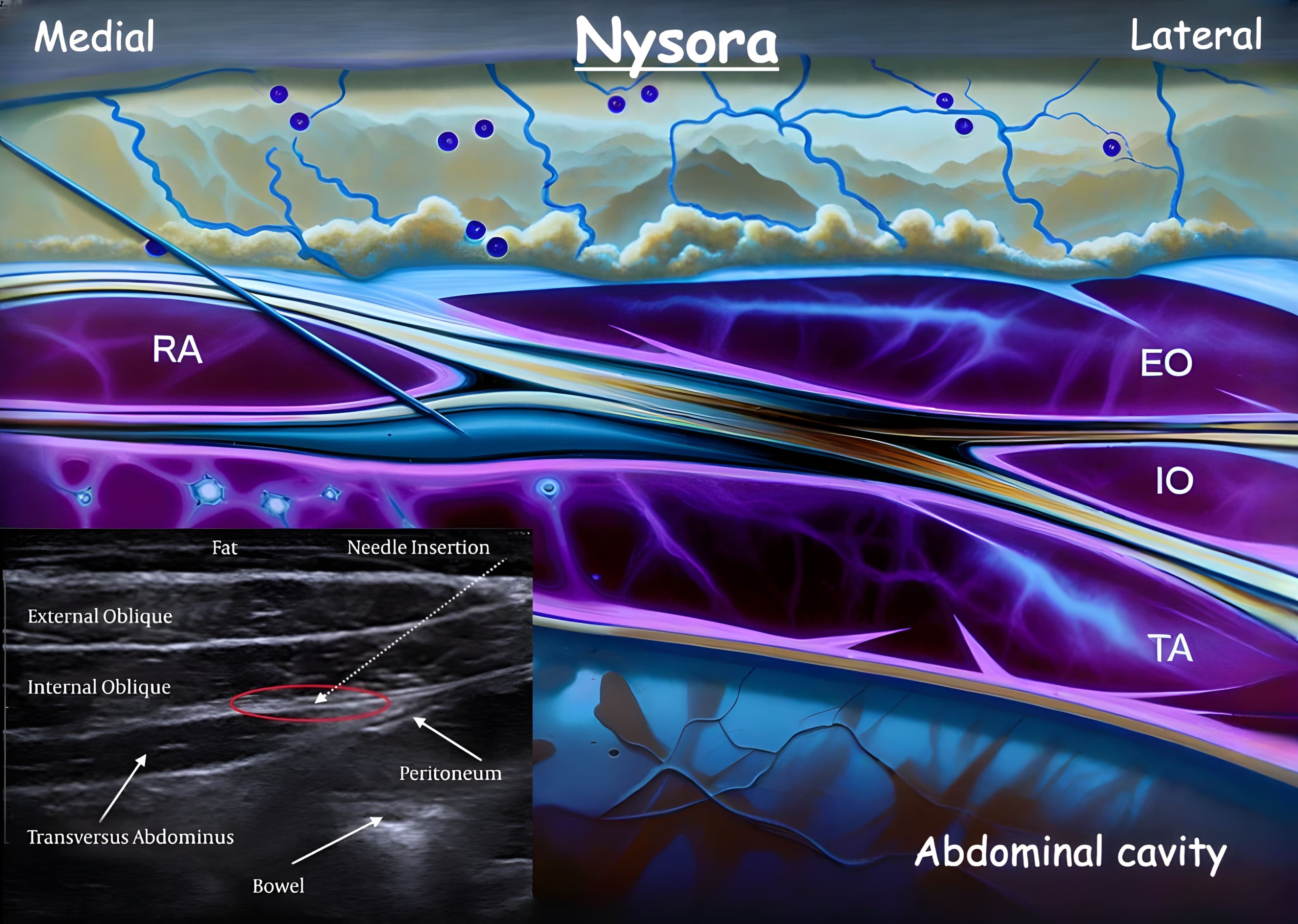
- Needle Insertion:
After identifying the layers, perform an in-plane needle insertion relative to the probe. For a lateral TAP block, the needle is usually introduced from the anterior (ventral) end of the probe and advanced in a lateral-posterior direction towards the plane between IO and TA.
Alternatively, the needle can be inserted from posterior to anterior – the key is to visualize the needle tip at all times. A blunt-tip block needle (e.g. 21–22G, 8–10 cm) is recommended to better feel the distinct “pops” as you penetrate each fascial layer and to reduce risk of organ perforation. Advance the needle through the external oblique and then the internal oblique; as the tip enters the TAP plane (deep to the IO, just above the transversus muscle), a subtle “give” or pop may be felt when the fascia is perforated.
- Hydrodissection and Injection:
Before injecting the full dose, it is prudent to confirm proper needle tip placement by hydrodissection – inject a small amount (1–2 mL) of normal saline or local anesthetic and observe the separation of the fascial plane on ultrasound. Correct placement is confirmed when the fluid is seen spreading and opening the space between the IO and TA muscles (appearing as a dark, lens-shaped pocket of fluid pushing the muscles apart).
If instead the fluid is intramuscular (causing a muscle to swell) or tracking superficially, adjust the needle tip position (withdraw or advance slightly) to get into the correct plane. Once the needle tip is in the TAP fascial plane, slowly inject the local anesthetic (LA) in increments with frequent aspiration to avoid intravascular injection. Typically about 15–20 mL is injected per side in an adult (see dosing below) to ensure sufficient spread.
Under ultrasound you will see the LA spreading anteriorly and posteriorly within the plane, elevating the transversus muscle away from the internal oblique. The goal is to deposit a broad field of LA that will “unzip” the plane and bathe the nerve branches in that interfascial space.
Approach Variations
There are a few variations of the TAP block technique depending on the surgical site:
Lateral (Midaxillary) TAP: Described above, with probe at midaxillary line between costal margin and iliac crest. This is the classic approach covering roughly T10–T12 dermatomes (umbilical area and below). Indicated for most lower abdominal surgeries (appendectomy, hysterectomy, etc.).
Subcostal TAP: Probe is placed more anterior, just below the costal margin (near the anterior axillary line or more medially) to target the TAP plane beneath the rectus abdominis sheath. The needle is inserted near the lateral border of the rectus muscle and advanced in-plane beneath the rectus, depositing LA between the rectus sheath (posterior layer) and the transversus abdominis muscle. This approach blocks the upper abdominal wall (T6–T9 dermatomes) and is useful for upper abdominal incisions (e.g. open cholecystectomy, liver surgery, upper midline incisions).
Anterior (Ilioinguinal) TAP: Probe near the ASIS (anterior superior iliac spine), oriented toward the umbilicus. This targets the lower TAP near the ilioinguinal/iliohypogastric nerves (L1) – useful to supplement coverage of the suprapubic area or inguinal region. Only ~5–10 mL may be needed for this if targeting just the L1 nerves in that area.
Posterior TAP: Probe at midaxillary line but slid posteriorly toward the edge of the lumbar triangle of Petit (just anterior to latissimus dorsi). LA is deposited at the very posterior end of the TAP plane, near the border of quadratus lumborum muscle. This approach may allow some spread into the paravertebral space and can cover T9–T12 dermatomes; it has been used for flank surgeries like nephrectomy. (Notably, the QL block evolved from this posterior approach)
Local Anesthetic Volume and Dosage
TAP blocks are field (plane) blocks that rely on volume to cover the nerve branches over a large area. For adults, a typical dose is 15–20 mL of local anesthetic per side for a single-shot TAP block. Studies have shown a minimum of ~15 mL is needed for reliable spread and efficacy, with improved block success when injecting ≥15 mL. Common choices are 0.25%–0.5% bupivacaine or ropivacaine (or even dilute 0.25% bupivacaine in 20 mL volume).
Care must be taken to calculate the total LA dose if performing bilateral TAPs to avoid exceeding toxic doses, since potentially 30–40 mL of LA might be used in an adult. The TAP plane is well-vascularized (especially laterally near muscular branches), so there is risk of systemic absorption; aspirate frequently and stay within safe dosage limits. If using long-acting agents (bupivacaine, ropivacaine), remember the mg/kg toxic dose (e.g. bupivacaine ~2.5 mg/kg without epinephrine) and adjust concentration/volume accordingly. Adding epinephrine (1:200,000) can reduce peak absorption.
For pediatric patients, the volume is weight-based. A common regimen is 0.3–0.5 mL/kg per side of 0.25% bupivacaine (or equivalent), up to a maximum of ~20 mL per side. For example, a 20 kg child might receive 10 mL per side of 0.25% bupivacaine. Pediatric regional anesthesia guidelines often prefer the lower end (0.3 mL/kg) for infants and higher (0.5 mL/kg) for older children. Using ultrasound allows effective blockade with these volumes and helps avoid inadvertent intraperitoneal injection (which is especially important in small children where the abdominal wall is thinner).
Always calculate the total mg dose (volume × concentration) and ensure it’s below the toxic threshold for the child’s weight. In bilateral blocks or if additional local anesthetic (e.g. surgeon infiltration) is used, communicate the total local anesthetic used to prevent Local Anesthetic Systemic Toxicity (LAST).
Ultrasound Landmarks and Tips
- Muscle Layer Identification:
If difficulty visualizing layers, start with the probe more anterior (over rectus) and slide laterally; the three layers (EO, IO, TA) will become evident lateral to the semilunar line. In obese patients, distinguish real muscle fascia from echogenic striations in subcutaneous fat by always identifying layers from deep (peritoneum) to superficial.
- Needle Visibility:
Align the needle trajectory as perpendicular to the probe as possible to enhance visibility (the needle is best seen when its plane is at 90° to the ultrasound beam). Needle guide software or echogenic needle design can help in larger patients.
- "Double Pop" (Landmark technique):
Historically, TAP blocks were done by loss-of-resistance pops using the lumbar triangle of Petit as an external landmark (injecting between EO and IO, then IO and TA by feel).
Ultrasound has largely replaced this blind technique, but knowing the landmark: triangle of Petit (latissimus dorsi posteriorly, external oblique anteriorly, iliac crest base) can help approximate the correct location.
- Spread and Dermatomes:
A single lateral TAP injection typically covers T10–T12 levels (umbilicus ~T10). To cover higher (T6–T9), use a subcostal approach on each side in addition, or place the injection more medially under rectus (subcostal TAP).
To cover L1 (inguinal region), ensure the injection spreads low toward the ASIS, or perform an anterior TAP (ilioinguinal block) near the ASIS. Multi-injection techniques (subcostal + lateral) may be used for broad coverage.
- Continuous Catheters:
AP catheters can be placed for continuous analgesia. This involves threading an epidural-style catheter into the TAP plane after hydrodissection with saline, typically advancing ~5–7 cm beyond the needle tip.
Continuous infusion of a dilute LA can provide prolonged pain relief (with some studies suggesting comparable analgesia to epidural for lower abdominal surgery). Catheter techniques are useful in patients where epidurals are contraindicated or to avoid hypotension in obstetric patients post-C-section.
- Safety:
Always visualize the peritoneum and bowel to avoid intraperitoneal injection. Keep the needle tip in view to prevent puncturing deeper structures (liver, spleen, bowel). Using ultrasound guidance has greatly reduced complication rates compared to blind technique.
Nonetheless, reported complications (rare) include accidental bowel perforation, liver or spleen laceration (especially with subcostal approach if too medial), intravascular injection leading to LAST, and in some cases transient femoral nerve block if LA tracks into the iliac fascia (causing quadriceps weakness). Proper technique and dosing make TAP blocks very safe and effective.
Summary (TAP Block)
TAP Block Coverage: Somatic analgesia of the unilateral anterior abdominal wall (skin, muscles, parietal peritoneum) from approximately T6 or T7 down to L1 dermatomes. It does not cover visceral pain (no effect on intra-abdominal organ sensation).
Use Cases: Effective adjunct for postoperative pain in abdominal surgeries (C-section, hernia repair, appendectomy, gynecologic, urologic, laparoscopic surgeries, etc.), reducing opioid requirements. Can differentiate abdominal wall pain vs intra-abdominal pain in chronic pain diagnosis.
Ultrasound Technique: Identify EO, IO, TA muscles on ultrasound; inject local anesthetic between IO and TA (or between TA and rectus sheath for subcostal approach). Use ~15–20 mL LA in adults (per side) and 0.3–0.5 mL/kg in pediatrics. Always aspirate and observe proper spread separating the muscle layers.
Benefits: Provides unilateral abdominal wall numbness from costal margin to inguinal region, significantly improving postoperative comfort. Part of multimodal analgesia – associated with less opioid use and possibly less nausea. Especially useful when epidural is contraindicated or undesired (e.g. coagulopathy, outpatient surgery).
Limitations: TAP block is purely somatic; visceral pain (e.g. from bowel manipulation) may still require systemic analgesics unless a more extensive block (paravertebral or QL block) is done. Duration is limited to the local anesthetic used (typically ~12–18 hours with long-acting agents); continuous catheters can extend this.
Safety: Low complication rate under ultrasound guidance. Avoid intraperitoneal injection and monitor total local anesthetic dose to prevent systemic toxicity. TAP blocks, when correctly performed, have a high safety profile and are easy to learn, making them a popular choice in ERAS (enhanced recovery) protocols for abdominal surgery.